September 3, 2021

Neuroscientists at MIT and Massachusetts General Hospital have developed a statistical framework that rigorously describes the brain state changes that patients experience under ketamine-induced anesthesia
By developing the first statistical model to finely characterize how ketamine anesthesia affects the brain, a team of researchers at MIT’s Picower Institute for Learning and Memory and Massachusetts General Hospital have laid new groundwork for three advances: understanding how ketamine induces anesthesia; monitoring the unconsciousness of patients in surgery; and applying a new method of analyzing brain activity.
Based on brain rhythm measurements from nine human and two animal subjects, the new model published in PLOS Computational Biology defines the distinct, characteristic states of brain activity that occur during ketamine-induced anesthesia, including how long each lasts. It also tracks patterns of how the states switch from one to the next. The “beta-hidden Markov model” therefore provides anesthesiologists, neuroscientists, and data scientists alike with a principled guide to how ketamine anesthesia affects the brain and what patients will experience.
In parallel work the lab of senior author Emery N. Brown, an anesthesiologist at MGH and Edward Hood Taplin Professor of Computational Neuroscience at MIT, has developed statistical analyses to characterize brain activity under propofol anesthesia, but as the new study makes clear, ketamine produces entirely different effects. Efforts to better understand the drug and to improve patient outcomes therefore depend on having a ketamine-specific model.
“Now we have an extremely solid statistical stake in the ground regarding ketamine and its dynamics,” said Brown, a professor in MIT’s Department of Brain and Cognitive Sciences and Institute for Medical Engineering & Science, as well as at Harvard Medical School.
Making a model
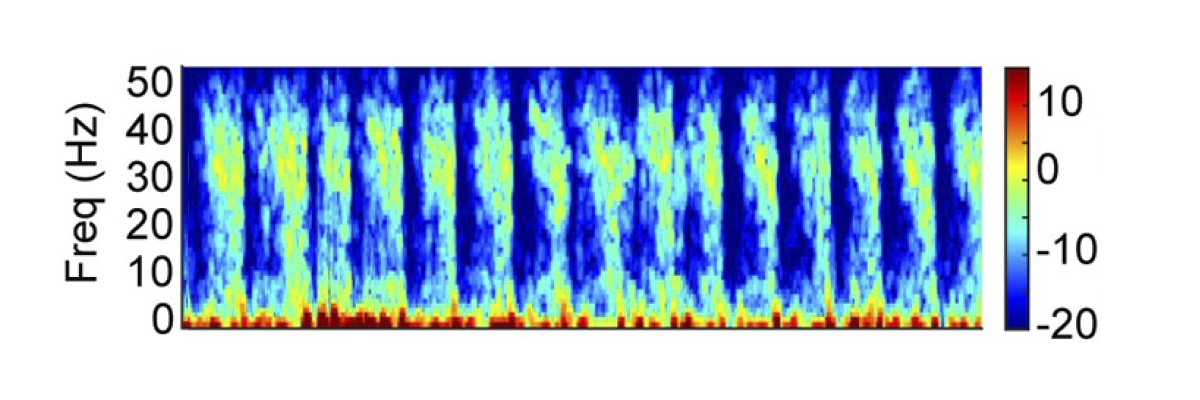
After colleagues at MGH showed alternating patterns of high-frequency gamma rhythms and very low-frequency delta rhythms in patients under ketamine anesthesia, Brown’s team, led by graduate student Indie Garwood and postdoc Sourish Chakravarty set out to conduct a rigorous analysis. Chakravarty suggested to Garwood that a hidden Markov model might fit the data well because it is suited to describing systems that switch among discrete states.
To conduct the analysis, Garwood and the team gathered data from two main sources. One set of measurements came from forehead-mounted EEGs on nine surgical patients who volunteered to undergo ketamine-induced anesthesia for a period of time before undergoing surgery with additional anesthetic drugs. The other came from electrodes implanted in the frontal cortex of two animals in the lab of Earl Miller, Picower Professor of Neuroscience at MIT.
Analysis of the readings with the hidden Markov model, using a beta distribution as an observation model, not only captured and characterized the previously observed alternations between gamma and delta rhythms, but a few other more subtle states that mixed the two rhythms.
Importantly, the model showed that the various states move through a characteristic order and defined how long each state lasts. Garwood said understanding these patterns allows for making predictions much in the same way that a new driver can learn to predict traffic lights. For instance, learning that lights change from green to yellow to red and that the yellow light only lasts a few seconds can help a new driver predict what to do when coming to an intersection. Similarly, anesthesiologists monitoring rhythms in a patient can use the findings to ensure that brain states are changing as they should, or make adjustments if they are not.
Characterizing the patterns of brain states and their transitions will also help neuroscientists better understand how ketamine acts in the brain, Brown added. As researchers create computational models of the underlying brain circuits and their response to the drug, he said, the new findings will give them important constraints. For instance, for a model to be valid, it should not only produce alternating gamma and slow rhythm states but also the more subtle ones. It should produce each state for the proper duration and yield state transitions in the proper order.
“Lacking this model was preventing some of our other work from going forward in a rigorous way,” Garwood said. “Developing this method allowed us to get that quantitative description that we need to be able to understand what’s going on and what sort of neural activity is generating these states.”
New ideas
As neuroscientists learn more about how ketamine induces unconsciousness from such efforts, one major implication is already apparent, Brown said. Whereas propofol causes brain activity to become dominated by very low-frequency rhythms, ketamine includes periods of high power in high frequency rhythms. Those two very different means of achieving unconsciousness seems to suggest that consciousness is a state that can be lost in multiple ways, Brown said.
“I can make you unconscious by making your brain hyperactive in some sense, or I can make you unconscious by slowing it down,” he said. “The more general concept is there’s a dynamic—we can’t define it precisely—which is associated with you being conscious and as soon as you move away from that dynamic by being too fast or too slow, or too discoordinated or hypercoordinated, you can be unconscious.”
In addition to considering that hypothesis, the team is looking at several new projects including measuring ketamine’s effects across wider areas of the brain and measuring the effects as subjects awaken from anesthesia.
Developing systems that can monitor unconsciousness under ketamine anesthesia in a clinical setting will require developing versions of the model that can run in real-time, the authors added. Right now, the system can only be applied to data post-hoc.
In addition to Garwood, Chakravarty, Brown and Miller, the paper’s other authors are Jacob Donoghue, Meredith Mahnke, Pegah Kahali, Shubham Chamadia, and Oluwaseun Akeju.
The National Institutes of Health, the National Science Foundation, MGH, and the JPB Foundation provided funding for the study.



